In the last years, prosthetic techniques have gained increased interest in post oncological reconstruction and in congenital defect treatment. Both the fuctional and the aesthetic characteristics of the prosthesis are crucial, in view of allowing the patient to overcome the social, psychological and economic problems deriving from their handicap.
Traditional reconstruction techniques present a number of lacks: the patient’s discomfort and stress, the inaccuracy of the replicas, and the dependence on the artistic skills of an experienced prosthetist. In addition, the mould production process is cumbersome, and time consuming. Finally, the overall process is not adaptive, i.e., whenever the existing prothesis should be replaced, the overall process must be carried out from scratch.
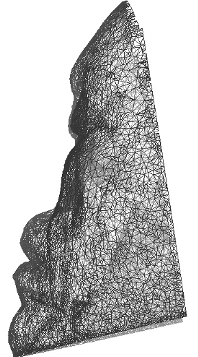
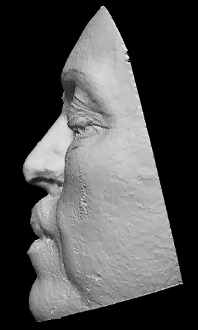
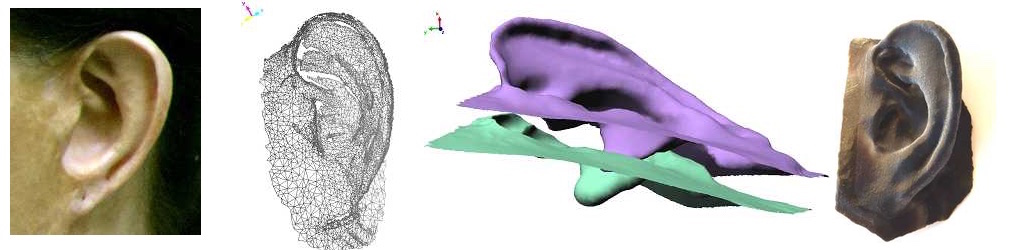
The purpose of this research activity is to develop a novel approach that combines optical three-dimensional acquisition, reverse engineering (RE) and rapid prototyping (RP) for the prosthetic reconstruction of facial prostheses.
Relevant Publications
Sansoni, G.; Cavagnini, G.; Docchio, F.; Gastaldi, G. “Virtual and physical prototyping by means of a 3D optical digitizer: application to facial prosthetic reconstruction“, Virtual and Physical Prototyping, Vol. 4, pp. 217-226. 2009
Sansoni, G.; Trebeschi, M.; Cavagnini, G.; Gastaldi, G. “3D Imaging acquisition, modeling and prototyping for facial defects reconstruction“, Proceedings of SPIE Three-Dimensional Imaging Metrology, Vol. 7239, pp. 1-8. 2009
Cavagnini, G.; Sansoni, G.; Vertuan, A.; Docchio, F. “3D optical Scanning: application to forensic medicine and to maxillofacial reconstruction“, Proceedings of International Conference on 3D Body Scanning Technologies, pp. 167-178. 2010